Patellar Maltracking and Subluxation
Pathophysiology and Etiology
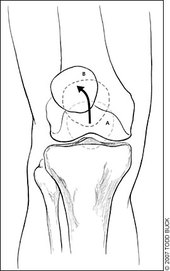
Patellar maltracking is more common with lateral tracking (vs medial) within the trochlear groove of the femur. It is also common in conjunction with a lateral tilt and upward rotation of the patella of the superior lateral border of the patella. The term subluxation is used when the patella temporarily tracks past the trochlear groove laterally, commonly an increase in severity than patellar maltracking. Prolonged maltracking of the patella will likely result in chondromalacia
See chondromalacia for progression of continued chronic patellar maltracking
The etiology continues to be an open debate, with populations who are asymptomatic that show signs and symptoms of patellar maltracking/subluxation.
Yet, these are the associations of causing anterior knee pain with patellar maltracking:
See chondromalacia for progression of continued chronic patellar maltracking
The etiology continues to be an open debate, with populations who are asymptomatic that show signs and symptoms of patellar maltracking/subluxation.
Yet, these are the associations of causing anterior knee pain with patellar maltracking:
- Direct trauma to the patella medially or laterally causing subluxation
- General joint hypermobility (Sheehan et al)
- Increased Tibiofemoral internal rotation (Sheehan et al 2008)
- Increase Q angle
- Patella alta (Frosch et al 2011, Sheehan et al 2008)
- Trochlear dysplasia (Frosch et al 2011)
- High tibial tuberosity trochlear groove distance (Frosch et al 2011)
- Lesion of the medial retinaculum/Medial patellofemoral ligament/Medial Collateral
- Length-tension relationships
- Shortened (tight) structures including tensor fascia latae (TFL), iliotibial band (ITB), hip flexors, hamstrings, vastus lateralis (VL) and lateral retinaculum
- Lengthened (weak) structures including vastus medialis obliques (VMO) and medial retinaculum
- VMO activation delay during gait compared contralaterally
- VMO and VL ratio (VL > VMO)
Diagnostic Tools
Observation/palpation bilaterally of patella protruding and tracking laterally compared to contralateral side with:
Weight bearing (squatting) and non-weight bearing (sitting with knees hanging)
Magnetic Resonance Imaging (MRI)
Weight bearing (squatting) and non-weight bearing (sitting with knees hanging)
- Static [knee flexion/extension between 0-30 degrees (terminal knee extension)] (Draper et al 2010)
- Dynamic (passive and active knee flexion/extension)
- “J Sign” Test – Excessive medial tracking at terminal extension with squatting
- Patella Glide Test – Pain with medial and/or lateral translation of the patella
- Patella Tilt Test – Assessing for tightness/laxity of medial/lateral attachments
- Ober’s Test – Assessing for ITB tightness
- Modified Thomas Test – Assessing for hip flexor, quadriceps and ITB tightness.
Magnetic Resonance Imaging (MRI)
Signs and Symptoms
Sharp anterior knee pain
Observation of lateral patellar tracking during beginning of flexion in weight bearing and non-weight bearing at terminal knee extension
Pain arising with highly loaded activities
Knee giving out with activity (related to subluxation)
Inhibiting quadriceps activity (severe subluxation or possible dislocation)
Inhibiting knee flexion
Possible edema, crepitation and locking of the knee
Observation of lateral patellar tracking during beginning of flexion in weight bearing and non-weight bearing at terminal knee extension
Pain arising with highly loaded activities
- Squatting
- Ascending/descending stairs
- Running
- Jumping
- Cycling
Knee giving out with activity (related to subluxation)
Inhibiting quadriceps activity (severe subluxation or possible dislocation)
Inhibiting knee flexion
Possible edema, crepitation and locking of the knee
Prognosis
The path of recovery depends on a combination of individual predisposition related to behaviors including activities of daily living (ADLs) and the multi-factorial structures involving the biomechanics of the patella. Prognosis can be good with an encompassing approach of further prevention, maintenance and rehabilitating the structures involved causing the abnormal patellar tracking. (eg. strengthening and shortening medial structures of the knee and lengthening of the lateral structures)
References
Andrish J. The management of recurrent patellar dislocation. Orthop Clin North Am 2008; 39(3): 313-327.
Arendt EA, Fithian DC, Cohen E. Current concepts in lateral patella dislocation. Clin Sports Med 2002; 21(3): 499-519.
Draper CE, Besier TF, Fredercison M et al. Differences in patellofemoral kinematics between weight-bearing and non-weight-bearing conditions in patient with patellofemoral pain. J Orthop Res 2011; 29:312–317.
Fithian DC, Paxton EW, Stone ML, et al. Epidemiology and natural history of acute patellar dislocation. Am J Sports Med 2004; 32(5): 1114-1121.
Frosch S, Balcarek P, Walde TA et al. The treatment of patellar dislocation: a systematic review. Z Orthop Unfall 2011 Dec; 1249(6):630-45.
Greiwe RM, Saifi C, Ahmad CS, Gardner TR. Anatomy and biomechanics of patellar instability. Oper Tech Sports Med 2010; 18(2): 62-67.
Koeter S, Diks MJF, Anderson PG, et al. A modified tibial tubercle osteotomy for patellar maltracking: Results at two years. J Bone Joint Surg Br February 2007; 89-B:180-185.
Pal S, Draper CE, Fredericson M et al. Patellar maltracking correlates with vastus medialis delay in patellofemoral pain patients. Am J Sports Med 2011; 39:590
Sheehan FT, Derasari A, Fine KM, Brindle TJ, Alter KE. Understanding patellofemoral pain with maltracking in the presence of joint laxity: Complete 3D in vivo patellofemoral and tiobiofemoral kinematics. J Orthop Res 2009; 27:561–570.
Arendt EA, Fithian DC, Cohen E. Current concepts in lateral patella dislocation. Clin Sports Med 2002; 21(3): 499-519.
Draper CE, Besier TF, Fredercison M et al. Differences in patellofemoral kinematics between weight-bearing and non-weight-bearing conditions in patient with patellofemoral pain. J Orthop Res 2011; 29:312–317.
Fithian DC, Paxton EW, Stone ML, et al. Epidemiology and natural history of acute patellar dislocation. Am J Sports Med 2004; 32(5): 1114-1121.
Frosch S, Balcarek P, Walde TA et al. The treatment of patellar dislocation: a systematic review. Z Orthop Unfall 2011 Dec; 1249(6):630-45.
Greiwe RM, Saifi C, Ahmad CS, Gardner TR. Anatomy and biomechanics of patellar instability. Oper Tech Sports Med 2010; 18(2): 62-67.
Koeter S, Diks MJF, Anderson PG, et al. A modified tibial tubercle osteotomy for patellar maltracking: Results at two years. J Bone Joint Surg Br February 2007; 89-B:180-185.
Pal S, Draper CE, Fredericson M et al. Patellar maltracking correlates with vastus medialis delay in patellofemoral pain patients. Am J Sports Med 2011; 39:590
Sheehan FT, Derasari A, Fine KM, Brindle TJ, Alter KE. Understanding patellofemoral pain with maltracking in the presence of joint laxity: Complete 3D in vivo patellofemoral and tiobiofemoral kinematics. J Orthop Res 2009; 27:561–570.
