Meniscal Tear
Pathophysiology and Etiology
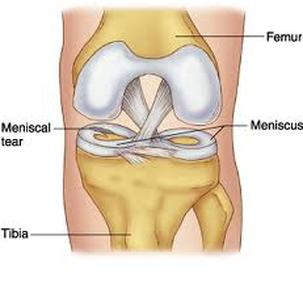
The menisci are C-shaped wedges of fibrocartilage located between the femoral condyles and tibial plateau. Each knee contains a medial and lateral meniscus that act as ‘shock absorbers’ between the femur and tibia, and help to both stabilize and cushion the knee joint. Meniscal tears are one of the most common knee injuries, especially for athletes who participate in contact sports, like football, soccer, basketball, and other similar sports. In sports-related meniscal tears, it is not uncommon for ligament injuries at the anterior-cruciate ligament (ACL) and medial collateral ligament to also occur. This pattern of injury is commonly referred to as the “unhappy triad”. A meniscal lesion was shown to occur at the same time of traumatic ACL rupture and/or further damage to the meniscus occurred during ACL insufficiency.1 Tandogan et al. have shown that the incidence of a meniscal tear, involving the medial (37%), lateral (16%), or both menisci (20%), that accompanied ACL tears is approximately 73%.2
The most common mechanism of injury in traumatic type meniscal tears occurs when the knee joint is flexed and the knee then undergoes a ‘twisting’ or rotational force through a weight-bearing limb. Other types of mechanisms of injury for the traumatic meniscal tear occur when the knee is flexed and either an external valgus (medical meniscus involvement) or varus (lateral meniscus involvement) is applied. Lee et al have shown that the incidence of medial meniscus tears is higher than lateral meniscus tears.3 They suggest that this is due to the more firmly attached medial meniscus and the greater amount of traumatic valgus force injuries during contact sports. Degenerative changes in cartilage associated with age can also result in a meniscus tear. Meniscal tears can be classified into different grades based on magnetic resonance imaging (MRI) signal. Crues et al have shown that grades 1 and 2 are typically asymptomatic and found in otherwise healthy knees while grade 3 tears are clinically significant meniscal tears.4 Meniscal tears can also be classified by the type of tear pattern present.5 These include the following:
The most common mechanism of injury in traumatic type meniscal tears occurs when the knee joint is flexed and the knee then undergoes a ‘twisting’ or rotational force through a weight-bearing limb. Other types of mechanisms of injury for the traumatic meniscal tear occur when the knee is flexed and either an external valgus (medical meniscus involvement) or varus (lateral meniscus involvement) is applied. Lee et al have shown that the incidence of medial meniscus tears is higher than lateral meniscus tears.3 They suggest that this is due to the more firmly attached medial meniscus and the greater amount of traumatic valgus force injuries during contact sports. Degenerative changes in cartilage associated with age can also result in a meniscus tear. Meniscal tears can be classified into different grades based on magnetic resonance imaging (MRI) signal. Crues et al have shown that grades 1 and 2 are typically asymptomatic and found in otherwise healthy knees while grade 3 tears are clinically significant meniscal tears.4 Meniscal tears can also be classified by the type of tear pattern present.5 These include the following:
- Bucket-handle/vertical tears
- Complex/degenerative tears
- Flap or parrot-break tears
- Horizontal cleavage tears
- Peripheral/longitudinal tears
- Radial tears
- Locked fragments
- Ruptured fragments
Diagnostic Tools
Meniscal tears can be accurately diagnosed by the patient’s history and mechanism of injury, through a thorough physical examination, and by the appropriate diagnostic imaging. If a meniscal tear is suspected, a MRI will likely be ordered to confirm the results of the patient’s physical examination and history. MRI in diagnosing medial and lateral meniscal tears has been shown to be nearly 89% accurate.6 Knee arthroscopy can be done to allow a quick diagnosis and treatment immediately after for more obvious cases of meniscal tears. An X-ray of the knee may be taken in order to rule out an acute pathology and to assess for any degenerative changes that may be occurring. During the physical examination the following tests can help rule in or out the presence of a meniscal tear:
- The McMurray test – pressing along the joint line while stress is placed on knee by alternating flexion and extension with varus or valgus stress.
- The Appley test – a grinding, compression maneuver that place the patient in prone and the knee at 90 degrees.
- Thessaly’s test – while standing on one leg the knee is bent to 20 degrees. The patient then rotates the knee internally and externally.
- Other tests include: Ege’s test, bounce home test, and Wilson test which are not as commonly used.
Signs and Symptoms
- Signs and symptoms of meniscal tears include:
- Patient reports mechanical symptoms, like locking, catching, or popping
- Mild to severe pain that worsens when the knee bears weight
- Swelling may be present
- Tenderness along joint line
- A positive sign on any of the previously mentioned special tests indicated by pain with clicking, locking, or popping
- Positive Cooper’s sign (patients commonly complain of pain in the knee when turning over in bed at night)
Prognosis
Non-surgical tears: Minor meniscal tears including grades 1 and 2 can expect to return to sport or activity in approximately 2 to 4 weeks with conservative rehabilitation. Moderate meniscal tears including more involved grade 2 tears can expect to return to sport or activity in approximately 4-6 weeks or even longer with conservative rehabilitation.
Post-surgical tears: Meniscal tears that are managed using surgical repairs can expect to return to sport or activity in 6 to 8 weeks or longer with conservative rehabilitation. As with many meniscal tear cases, the rehabilitation time may be longer if other knee structures, like the ACL or MCL, are involved as well.
Post-surgical tears: Meniscal tears that are managed using surgical repairs can expect to return to sport or activity in 6 to 8 weeks or longer with conservative rehabilitation. As with many meniscal tear cases, the rehabilitation time may be longer if other knee structures, like the ACL or MCL, are involved as well.
References
- Seitz H, Marlovits S, Wielke T, Vecsei V. [Meniscus lesions after isolated anterior cruciate ligament rupture]. Wien Klin Wochenschr. 1996;108(22):727-730.
- Tandogan RN, Taser O, Kayaalp A, et al. Analysis of meniscal and chondral lesions accompanying anterior cruciate ligament tears: relationship with age, time from injury, and level of sport. Knee Surg Sports Traumatol Arthrosc. 2004;12(4):262-270. Epub 2003 Sep 2020.
- Lee JJ, Choi YJ, Shin KY, Choi CH. Medial meniscal tears in anterior cruciate ligament-deficient knees: effects of posterior tibial slope on medial meniscal tear. Knee Surg Relat Res. 2011;23(4):227-230. Epub 2011 Nov 2030.
- Crues JV, 3rd, Mink J, Levy TL, Lotysch M, Stoller DW. Meniscal tears of the knee: accuracy of MR imaging. Radiology. 1987;164(2):445-448.
- Dandy DJ. The arthroscopic anatomy of symptomatic meniscal lesions. J Bone Joint Surg Br. 1990;72(4):628-633.
- Yan R, Wang H, Yang Z, Ji ZH, Guo YM. Predicted probability of meniscus tears: comparing history and physical examination with MRI. Swiss Med Wkly. 2011;141:w13314.(doi):10.4414/smw.2011.13314.
- Fabricant PD, Jokl P. Surgical outcomes after arthroscopic partial meniscectomy. J Am Acad Orthop Surg. 2007;15(11):647-653.
- Northmore-Ball MD, Dandy DJ, Jackson RW. Arthroscopic, open partial, and total meniscectomy. A comparative study. J Bone Joint Surg Br. 1983;65(4):400-404.
