Patellofemoral Pain Syndrome
Treatment

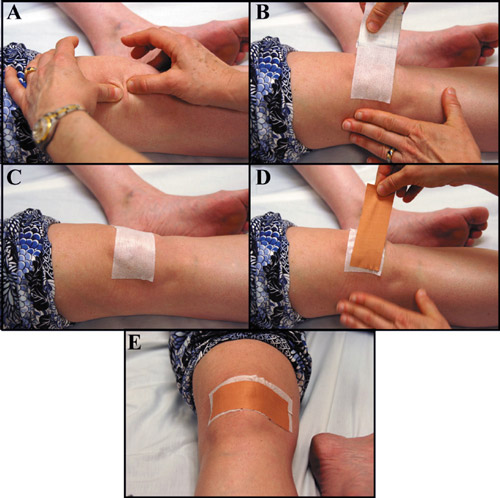
When treating patellofemoral pain syndrome (PFPS) “possibilities for interventions are numerous, but no general consensus exists as to the most efficacious treatment approach. Current evidence-based treatment approaches include taping, strengthening of the hip musculature and quadriceps, manual therapy to the lower quarter, and fitting of foot orthoses.”4 Additionally, Iverson et al., found that “Patients with PFPS who demonstrate a side-to-side difference in hip internal rotation range of motion greater than 14 degrees and are treated with a lumbopelvic manipulation have an 80% posttest probability of experiencing a positive outcome.”3 The rationale behind a lumbopelvic manipulation is that studies have shown that it decreases quadriceps inhibition in involved knees. While taping is a commonly recommended intervention “multiple studies have shown patellar taping to decrease pain and, theoretically, to improve patellar tracking by changing vastus medialis obliquus timing with functional tasks, while other researchers have shown that there is no difference in pain or patellar alignment with sham versus directional taping.”4 Therefore, the decision to use taping should be based on clinical expertise and patient preference. While strength training targeting the quadriceps musculature, specifically the vastus medialis obliquus, has been commonly used for treating PFPS, “it is unknown if the VMO can preferentially be recruited with exercise or if VMO atrophy is an indication of total quadriceps atrophy.”4 Additionally, weakness at the hip and gluteals have been associated with the development of PFPS as “recent studies have shown that there is weakness of the gluteus medius, gluteus maximus, and hip external rotators and poor proprioceptive control in patients with PFPS.”4 Interventions therefore should also focus on correcting these impairments as “there is evidence that treating hip muscle weakness can reduce PFPS.”1 Powers et al. also found that “bracing may help prevent PFPS.”1 In conclusion, there are a lot of proposed interventions for treating PFPS, and “despite extensive research, there is still little consensus as to the most effective treatment strategy for the management of patients with PFPS.”4
Prevention
According to Lankhorst et al, “the first step toward prevention is identification of possible risk factors or factors associated with PFPS.”5 In order to identify these risk factors, the authors conducted a systematic review. In that review they found that being female and having lower knee extension strength may be risk factors for the future development of PFPS.”5 In addition to taking steps to minimize the impact of risk factors, prevention should also include general conditioning, stretching, using proper equipment, using proper form, and activity modification. Additionally, the patient may need to undergo a weight reduction program to prevent the development of anterior knee pain.
Education
Education should include training on how to properly perform daily functional activities in a manner that will avoid placing stress on the patellofemoral joint. Additionally, the patient should also be given a home exercise plan to address impairments found during the initial examination and follow up treatments. Finally, the patient should be counseled about proper training techniques including gradual changes in intensity, frequency, and duration of exercise to allow the body to adapt to the increased workload.
References
1. Powers CM, Bolgla LA, Callaghan M, Collins N, Sheehan F. Patellofemoral pain: proximal, distal, and local factors, 2nd international research retreat. J Orthop Sports Phys Ther. 2012;42(6):A1-A54. Epub 2012 Jun 2011.
2. Barton CJ, Bonanno D, Levinger P, Menz HB. Foot and ankle characteristics in patellofemoral pain syndrome: a case control and reliability study. J Orthop Sports Phys Ther. 2010;40(5):286-296.
3. Iverson CA, Sutlive TG, Crowell MS, et al. Lumbopelvic manipulation for the treatment of patients with patellofemoral pain syndrome: development of a clinical prediction rule. J Orthop Sports Phys Ther. 2008;38(6):297-309; discussion 309-212. Epub 2008 Jan 2022.
4. Lowry CD, Cleland JA, Dyke K. Management of patients with patellofemoral pain syndrome using a multimodal approach: a case series. J Orthop Sports Phys Ther. 2008;38(11):691-702.
5. Lankhorst NE, Bierma-Zeinstra SM, van Middelkoop M. Risk factors for patellofemoral pain syndrome: a systematic review. J Orthop Sports Phys Ther. 2012;42(2):81-94. Epub 2011 Oct 2025.
2. Barton CJ, Bonanno D, Levinger P, Menz HB. Foot and ankle characteristics in patellofemoral pain syndrome: a case control and reliability study. J Orthop Sports Phys Ther. 2010;40(5):286-296.
3. Iverson CA, Sutlive TG, Crowell MS, et al. Lumbopelvic manipulation for the treatment of patients with patellofemoral pain syndrome: development of a clinical prediction rule. J Orthop Sports Phys Ther. 2008;38(6):297-309; discussion 309-212. Epub 2008 Jan 2022.
4. Lowry CD, Cleland JA, Dyke K. Management of patients with patellofemoral pain syndrome using a multimodal approach: a case series. J Orthop Sports Phys Ther. 2008;38(11):691-702.
5. Lankhorst NE, Bierma-Zeinstra SM, van Middelkoop M. Risk factors for patellofemoral pain syndrome: a systematic review. J Orthop Sports Phys Ther. 2012;42(2):81-94. Epub 2011 Oct 2025.
